Foram N. Ashar, Anna Moes, Ann Z. Moore, Megan L. Grove, Paulo H.M. Chaves, Josef Coresh, Anne B. Newman, Amy M. Matteini, Karen Bandeen-Roche, Eric Boerwinkle, Jeremy D. Walston, and Dan E. Arking.
Poster presented at the American Society of Human Genetics meeting, October 21st, 2014, in San Diego, CA. [Download PDF]
Abstract
Age-related declines in mitochondrial function have long been hypothesized to underlie multiple biological changes that increase vulnerability to multiple disease states, functional and cognitive decline, and ultimately, mortality. While the association of mitochondrial variants with age-related disorders is well-established, the effect of mtDNA copy number, which reflects energy reserves and oxidative stress, on aging and mortality in the general population has not been well studied. To address this gap, we examined mtDNA copy number in two large multi-center prospective studies—the Cardiovascular Health Study (CHS) and the Atherosclerosis Risk in Communities (ARIC) study—with a total of 16,401 samples of European and African descent focusing on two primary phenotypes—prevalent frailty in CHS, and all-cause mortality in ARIC and CHS.
In race-stratified meta-analyses, we demonstrate a significant inverse association of mtDNA copy number with age, with a reduction of 0.12 standard deviation units with a 10 year differences in age (P=2.78 x 10-25), and higher mtDNA copy number in women relative to men (meta-analysis OR=1.33, 95% CI 1.14-1.51, P=6.91 x 10-45). Furthermore, we show that lower mtDNA copy number is significantly associated with prevalent frailty in 4,109 self-identified white participants from CHS (OR=0.91, 95% CI, 0.85-0.97, P=0.005). Finally, mtDNA copy number is a strong predictor of all-cause mortality in an age and sex-adjusted, race-stratified analysis of 16,401 participants from both cohorts with a pooled hazard ratio of 1.47 (95% CI 1.33-1.62, P=4.24 x 10-14) for the lowest quintile of mtDNA copy number relative to the highest quintile. In summary, we report that a single, easily implemented measure of mtDNA copy number, isolated from whole blood decades before the event of interest (death), is predictive of all-cause mortality.
Cohorts and Methods
Cardiovascular Health Study (CHS)
- 4,108 self-identified white, and 784 black participants
- mtDNA copy number determined by multiplex Taqman assay carried out in triplicate, followed by quantile normalization across plates.
Atherosclerosis Risk In Communities (ARIC) study
- 9,025 self-identified white, and 2,484 black participants
- mtDNA copy number extracted from median mitochondrial probe intensity on Affymetrix arrays. This measure was adjusted for principal components generated from probe intensities of 1,000 nuclear probes to account for plate and batch effects.
Association of mtDNA copy number with prevalent frailty
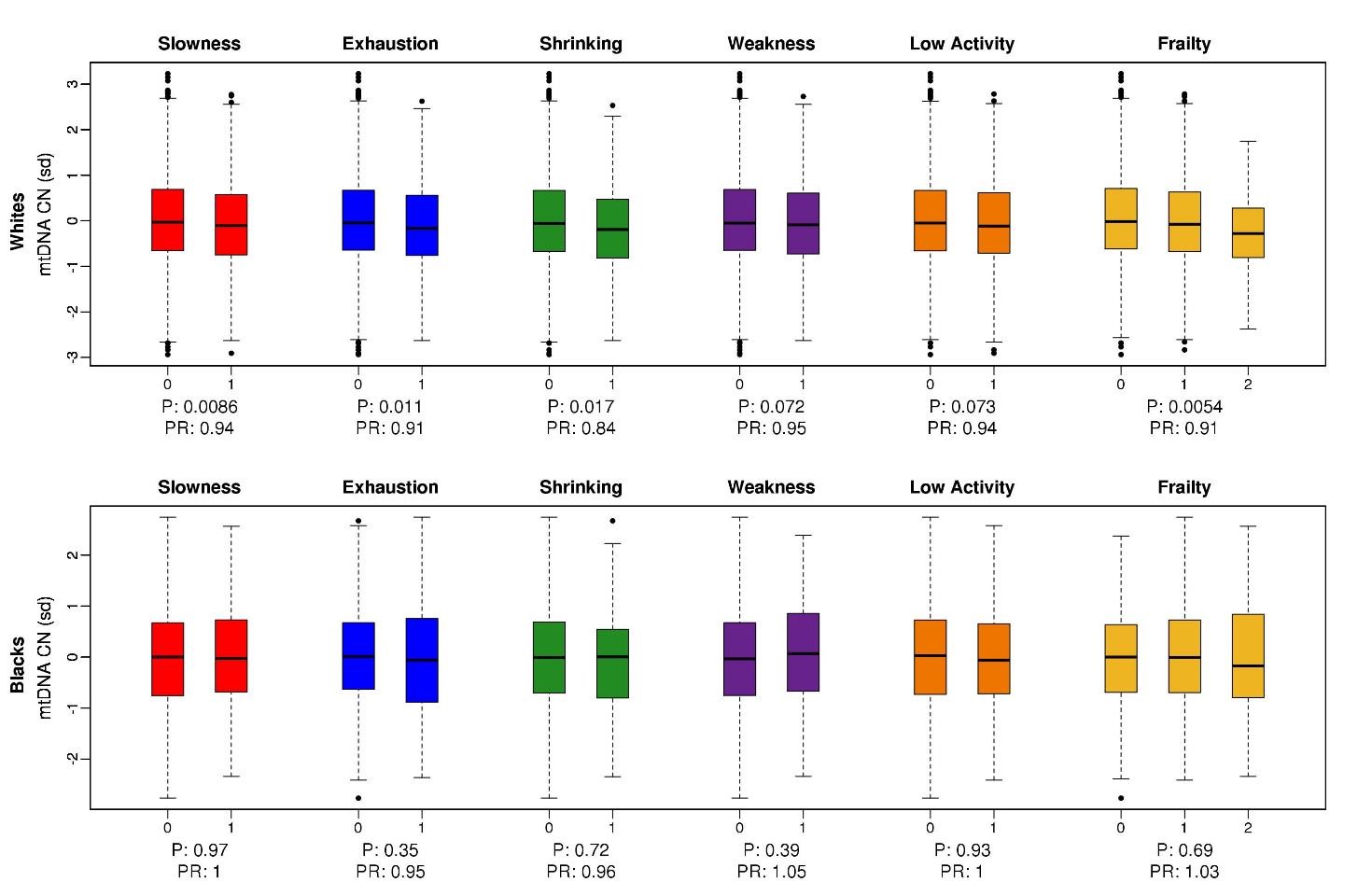
In a race-stratified analysis of samples from CHS, we observed a statistically significant association between lower mtDNA copy number and frailty, adjusted for age and sex, in whites. This association was not driven by any single component of the frailty phenotype, with three out of five frailty characteristics showing statistically significant association with lower mtDNA copy number in whites. While we observed this association in whites, we see no association of mtDNA copy number on any of the frailty characteristics in CHS blacks.
mtDNA copy number is a predictor of all-cause mortality
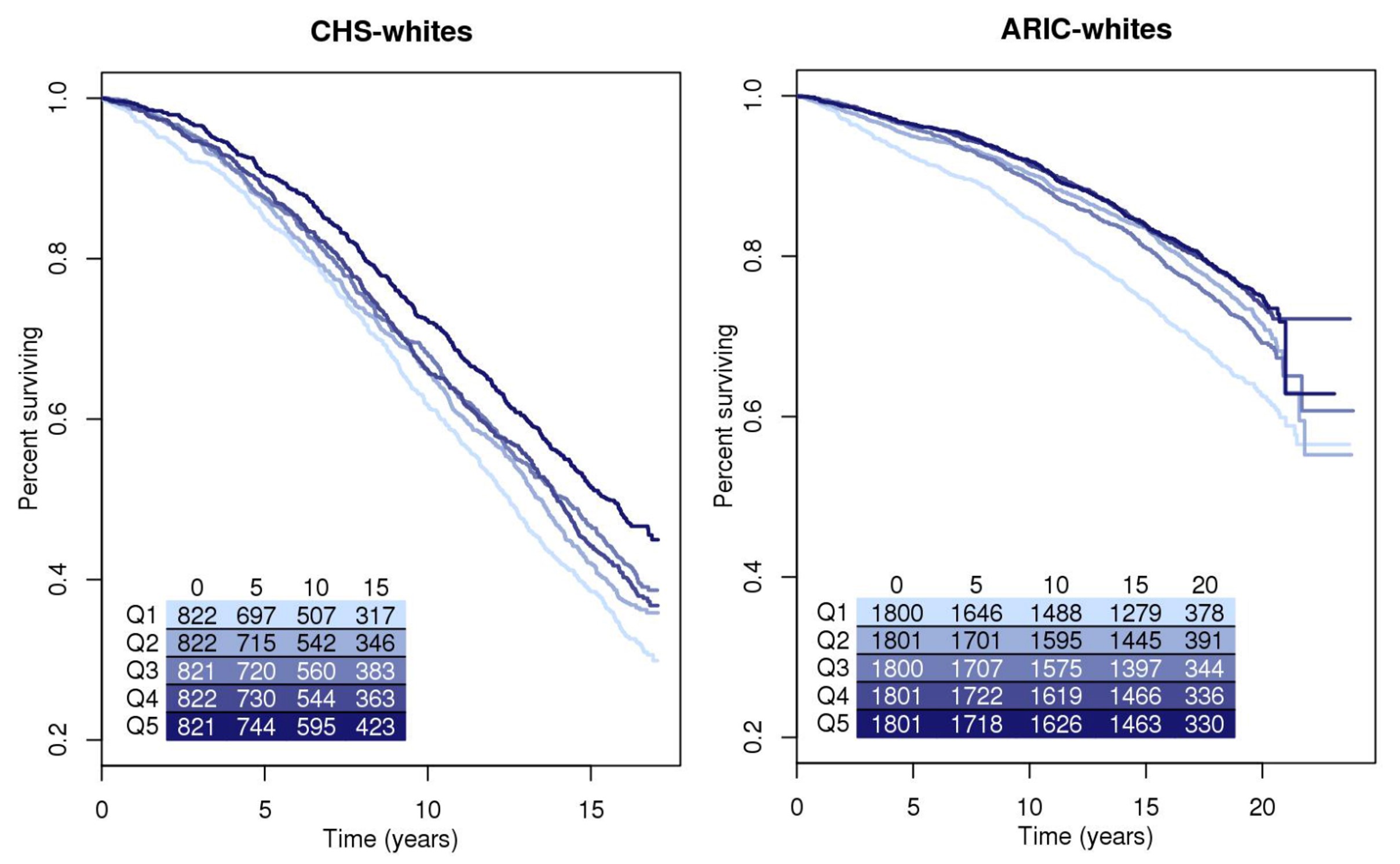
To assess the association of mtDNA copy number with mortality, we use a Cox proportional-hazards model, with quintiles of mtDNA copy number as the variable of interest, and age, sex, and collection site as additional covariates in the baseline model. In race-stratified analyses, we observed a statistically significant association between lower mtDNA copy number and mortality, in CHS whites, ARIC whites, and ARIC blacks.
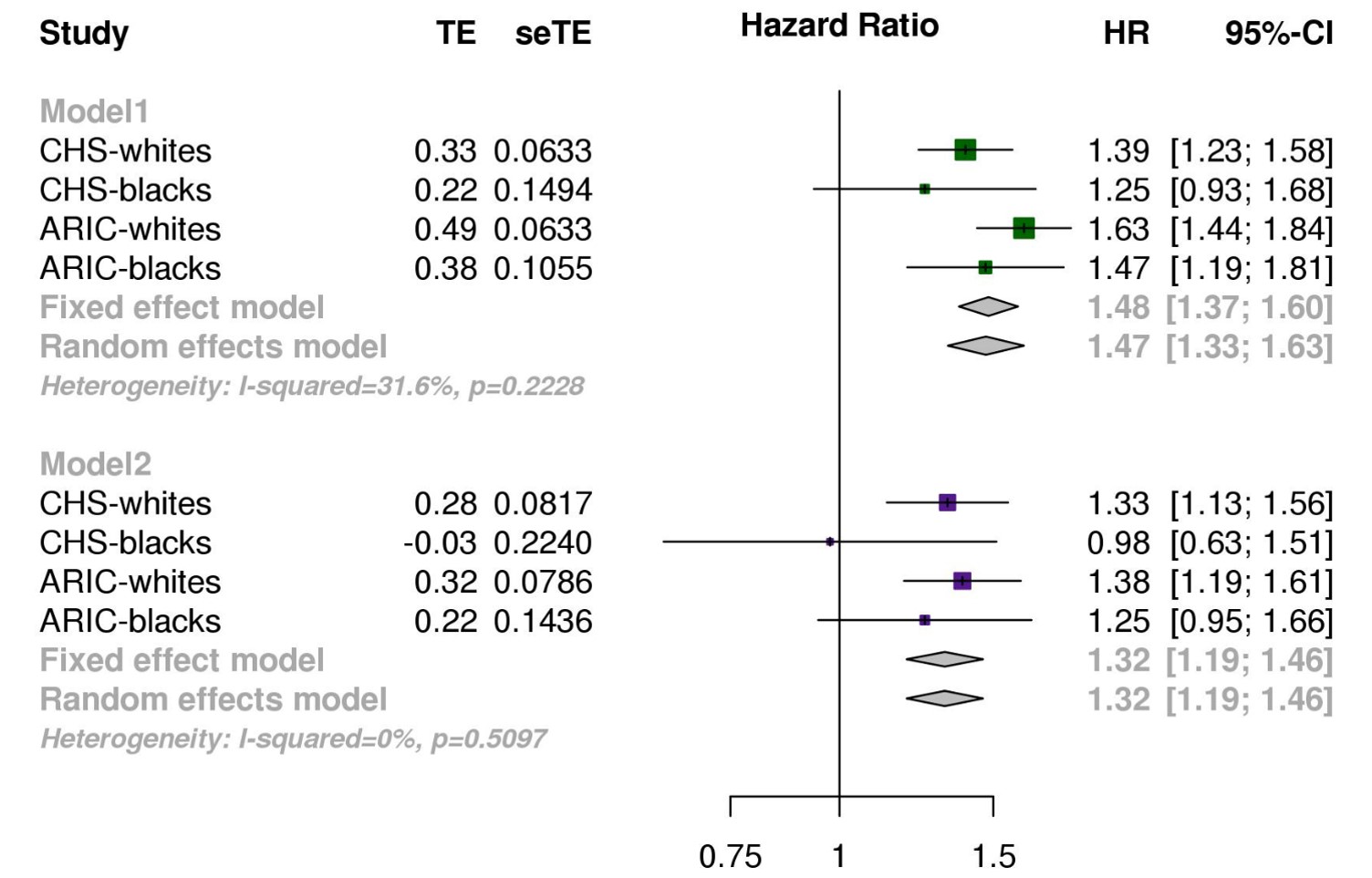
An inverse-variance weighted meta-analysis of race-stratified results from both cohorts for the age, sex and collection site adjusted effect of the lowest quintile relative to the highest quintile on mortality (Model 1), yielded an overall hazard ratio of 1.47 (95% CI, 1.33-1.62, P<0.001), with no significant heterogeneity between the subgroups (P=0.26)
Meta-analysis of a more stringent multivariate model adjusted for age, sex, collection center, BMI, HDL, total cholesterol, prevalent hypertension, and smoking status, and excluding all samples with prevalent CHD (Model 2), gave a meta-analyzed hazard ratio of 1.32 (95% CI, 1.19-1.46, P<0.001).
Conclusions
We demonstrate that low mtDNA copy number is strongly associated with age, sex, and frailty, and an independent predictor of mortality in 16,401 samples from two large multi-ethnic cohorts, even after adjustment for traditional mortality risk factors and exclusion of prevalent disease states associated with high risk of mortality.
Acknowledgments The authors thank the staff and participants of the ARIC and CHS studies for their important contributions This work was supported by the Johns Hopkins University Claude D. Pepper Older Americans Independence Center, National Institute on Aging, P30-AG021334, University of Pittsburgh Claude. D. Pepper Older Americans Independence Center P30-AG-024827. The Atherosclerosis Risk in Communities Study is carried out as a collaborative study supported by National Heart, Lung, and Blood Institute contracts (HHSN268201100005C, HHSN268201100006C, HHSN268201100007C, HHSN268201100008C, HHSN268201100009C, HHSN268201100010C, HHSN268201100011C, and HHSN268201100012C), R01HL087641, R01HL59367 and R01HL086694; National Human Genome Research Institute contract U01HG004402; and National Institutes of Health contract HHSN268200625226C. The authors thank the staff and participants of the ARIC study for their important contributions. Infrastructure was partly supported by Grant Number UL1RR025005, a component of the National Institutes of Health and NIH Roadmap for Medical Research. The Cardiovascular Health Study was supported by contracts HHSN268201200036C, HHSN268200800007C, N01 HC55222, N01HC85079, N01HC85080, N01HC85081, N01HC85082, N01HC85083, N01HC85086, and grant HL080295 from the National Heart, Lung, and Blood Institute (NHLBI), with additional contribution from the National Institute of Neurological Disorders and Stroke (NINDS). Additional support was provided by AG023629 from the National Institute on Aging (NIA).Contact Information
Foram Ashar
fashar1@jhmi.edu
Anna Moes
amoes1@jhmi.edu
Dan Arking
arking@jhmi.edu
www.arkinglab.org